

Custom Search
|


|
Dermpath-India Pathology of Seborrheic Keratosis Dr Sampurna Roy MD 2022
|

 |
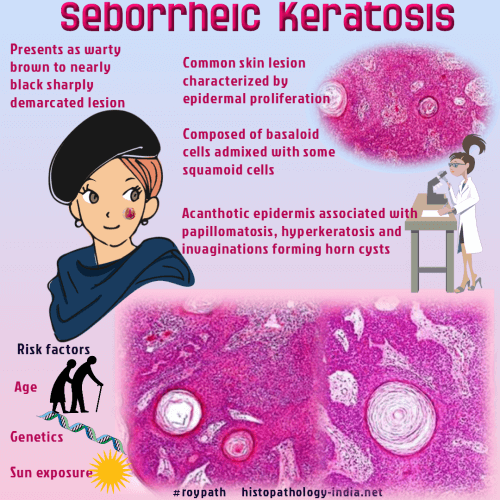
Seborrheic keratosis is a very common cutaneous lesion characterized by epidermal proliferation and composed of basaloid cells admixed with some squamoid cells. Clinically, these are often multiple lesions occuring in any part of the body except palms and soles. Common sites include trunk, arms and face in middle aged or elderly patients. In characteristic cases the lesions are warty in appearance, brown to nearly black, sharply demarcated. The lesion may look as if "stuck on" to the skin. Histological patterns: The tumour shows an elevated area of acanthotic epidermis associated with papillomatosis, hyperkeratosis and invaginations forming horn cysts. The tumour is usually symmetric at the level of the adjacent epidermis. There is an exophytic expansion. It is composed of broad interconnecting bands of cells containing the horn cysts. The tumour cells are similar to the basal cells of the epidermis and are called "basaloid" cells. Squamous cells form the other cellular component and are present in varying numbers. Hyperpigmentation of the basal layer is common. Based on architectural patterns seborrheic keratosis may be acanthotic, hyperkeratotic, reticular or verrucous forms. Within these general architectural patterns there are various growth patterns which may be uniform or mixed in any individual lesion. These include monomorphous, pleomorphic, clonal, fascicular and acantholytic.
Leser-Trélat is a rare paraneoplastic sign that is characterized by the sudden eruption of multiple seborrheic keratoses, associated with underlying internal malignancies. Similar non-malignancy-associated multiple seborrheic keratoses eruptions are referred to as the "pseudo-sign of Leser-Trélat".
|
|
|
|
|
