Custom Search
|
|
Custom Search
|
|
Infectious Disease Online Pathology of Histoplasmosis |

|
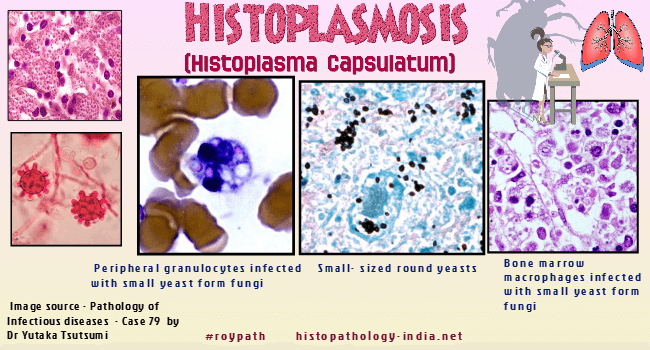
Histoplasmosis is caused by
infection with Histoplasma capsulatum.
Epidemiology: In the United States, Histoplasma mainly lives in the central and eastern states, especially areas around the Ohio and Mississippi River valleys. The fungus also lives in parts of Central and South America, Africa, Asia, and Australia. The fungus seems to grow best in soils having a high nitrogen content, especially those enriched with bird manure or bat droppings. Normal reservoir: Droppings of birds and bats & moist soil, particularly beneath trees. Mode of infection: Infection by this dimorphic soil fungus occurs by inhalation. Organisms reach alveolar spaces where it multiplies in mononuclear phagocytes. It is not contagious. Presentation: A- 90% human infections are asymptomatic and develop multiple calcification in lungs: B- Symptomatic patients (10%) are 3 types: 1. Acute pulmonary disease: Influenza-like symptoms develop after 7-15 days of infection and heals. In normal adults there is peripheral pulmonary lesion associated with hilar lymphadenopathy resembling Ghon's complex of tuberculosis. Small percentage of cases, develop fungemia. 2. Hematogenous spread: Mononuclear phagocytes (containing organisms) enter into various organs, mainly, in lungs, lymph nodes, spleen, liver, bone marrow, gastrointestinal tract and adrenals. In children and immunocompromised adults, particularly in HIV patients, it resembles primary tuberculosis with rapid dissemination like military tuberculosis. There is no granuloma formation. Collection of phagocytic cells with organisms are seen in the involved organs. Lesions are also seen in the nose, mouth, tongue & larynx. 3. Chronic pulmonary lesions with cavity: Lesions resemble tuberculosis for similar clinical & pathological features. Chronic cough, chest pain, night sweat, malaise, loss of weight etc are common in both patients. Cavity in upper lobe, is also seen in both the cases.
Microscopic features: Lung: Yeast-like forms in tissue section : 2 to 4 µm in diameter, uninucleate, spherical to oval; have single buds; and often situated in clusters . It is usually difficult to see the organisms on examination of Hematoxylin and eosin - stained sections, except in the acute or disseminated forms when organisms are numerous. A clear space or artifactual "halo" may be evident due to the retraction of the basophilic fungal cell cytoplasm from the poorly stained cell wall. Hyphae are extremely rare in tissue sections except in case of intravascular infections. Acute phase: Numerous organisms within alveolar spaces and the interstitium ; Acute fibrinous pneumonia without granulomatous inflammation ; organisms within macrophages ; a mononuclear infiltrate, followed by granulomatous inflammation ; Pulmonary nodule is a granuloma composed of central caseous necrosis surrounded by connective tissue containing epithelioid and multi-nucleated giant cells. Noncaseating granulomas may be seen: This may be the only finding on bronchoscopic biopsies. Differential diagnosis: Sarcoidosis. Chronic infection : Necrotizing granuloma ; heal by fibrosis (with a concentric laminar pattern) ; Fibrosing granulomas may calcify ; central necrotic areas may persist ; usually there are few organisms present the central necrotic area ; Necrotic centers may be lost in tissue processing. This may cause difficulty in identification of the organisms ; Chronic fibrosing cases may resemble reactivation tuberculosis. Disseminated form ( in patients with HIV infection) ; extensive tissue infiltration with many organisms. Skin: Granulomatous infiltrate in the dermis and sometimes subcutis ; Numerous parasitized macrophages containing yeast-like organisms ; Organism often has a surrounding clear halo; Langhan's giant cells, a few lymphocytes and plasma cells are also present ; In acute disseminated cases parasitized macrophages are more prominent. In HIV-positive patients inflammatory cell infiltrate is sparse. Healing lesions are characterized by fibrosis. African form - The organisms are larger in size. Foreign-body type of granulomatous reaction is present. Diagnosis: 1. Histoplasmin skin test-positive with negative tuberculin test. 2. Analysis of the organism in sputum, lung tissue, blood, cerebrospinal fluid (CSF), or bone marrow tissue. 3. Antigen tests performed on blood, urine, or CSF. 4. In chronic infection, special stains are usually necessary to identify the organisms and the Methenamine-Silver stain is the best. In chronic infections the organisms stain poorly with the PAS stain, but in acute infections with numerous organisms this stain is useful. 5. Direct immunofluorescence on histologic sections can help establish the diagnosis Visit: African Histoplasmosis (Histoplasma Duboisii)
|
|
|
Visit:- Dermatopathology Online
![]()
Copyright © 2022 histopathology-india.net